Home » Healthcare
Category Archives: Healthcare
Pandemic Voices Cannot Be Silenced
I am a surgeon. These are unprecedented times. The economy of our entire country was shut down to curb the spread of the Coronavirus. The number of those infected and the number who have died grow exponentially. The resources of our resource full United States are stretched thin as cities and states fight for personal protective equipment, ventilators and health care workers who are working constantly and exhausted.
Unlike war time, journalists cannot easily report from the front lines as they would use valuable protective gear. The public gets its stories from the hospital bedside and Intensive Care directly from health providers – the doctors, nurses, assistants, respiratory technologists, lab workers, cleaning staff.
Through their eyes and from their mouths come heartbreaking stories of sorrow, suffering and death.
Now healthcare administrators are censoring doctors and nurses for posting updates or talking to the news about their hectic work fighting this pandemic. Hospitals do not want to look bad or unprepared. Early in the pandemic, in some hospitals, employees were forbidden or punished for walking about with a mask – which apparently sent the wrong message of an uncontrolled crisis.
The Washington Post reported on a doctor in Bellingham, Washington who was fired for his Facebook post stating he and his staff did not have a sufficient supply of personal protective equipment. That Post author was also told not to share personal stories with the press. Other healthcare workers are warned to get permission from hospital administration, before speaking to the media.
Now many doctors and nurses are staying silent and refusing media requests for interviews and comment for fear of reprisal. Truly the Washington Post tagline “democracy dies in darkness” is apt.
We health providers know the HIPAA laws which protect patient privacy. We are not divulging protected patient health information. We are sharing stories of our ordeal battling this virus, crying out for more resources like personal protective equipment, voicing our frustration when we are placed in an uncomfortable situation. What does a gynecologist or orthopedic surgeon know about respiratory care and ventilator settings.
Hospitals and health systems want to protect their institutions and administrators want to protect their jobs.
We on the front line, want to save lives.
I hope that when this crises is over, health systems and hospitals will not retaliate against those who spoke up, using that excuse to trim their roster of troublemakers. I hope doctors and nurses and other providers will be united to protect those voices that rose up during this pandemic.
The Sad Tale of the USC Medical School Dean
It is unfortunate, that situation at USC Medical School, where the dean, Dr. Carmen A. Puliafito had been found in a Pasadena hotel room with a 21 year old woman in “provocative clothing” who overdosed on drugs. That happened in March 2016.
Allegations, pictures and even videos of Puliafito in the company of criminals and drug addicts had been popping up since 2015. There are many pictures of him enjoying recreational medicines. He was using methamphetamine and other drugs while serving as dean of the Keck School of Medicine. While there is nothing wrong with “partying”, the use of drugs and paying for prostitutes may be crossing the line.
It is sad, when a leader abuses his or her power and commits such errors in judgement. Why does this happen? Are they so high above the ordinary workers, do they make so much money that they feel infused with invincibility, are they beyond reproach, why do they suffer such ethical lapses?
Despite the vetting we mortal doctors go through to get privileges at a healthcare or teaching facility, why did USC not detect Puliafito’s ethical deficiencies? Too often, I hear that the institution reveres a candidate and after all, this one had a Wharton MBA. Institutions hate to insult candidates with pointed inquiries. Sometimes the little discovered nuggets of deficiency are considered just minor ethical oversights….we are all human.
So, this nonsense has been going on under USC’s nose for two years. I heard astonishingly, that USC is finally making plans to fire Puliafito. What? Another two year process?
If I was graduating from the USC Medical School, I am certain that Dean Puliafito will not be handing me my degree.
But he could be a hell of a party host that evening
The Future of Doctors
In the age of spiritual machines Ray Kurzweil in 2001 predicted:
By 2020, a $1,000 computer will match processing speed of the human brain – 20 billion calculations per second
By 2030 it will simulate the brain power of a small village about 1,000 human minds
By 2048 it will have the brain power of the entire population of the US.
I predict that within 20-30 years the computer will replace the venerable physician. Computers can already be programmed to detect sarcasm and read emotions. They can study your face and body language. Computerized psychotherapists or cybertherapy is soon to come. Programs can detect deviation from the standard pattern of human physiology, thinking and behavior. We can already program standards of care and integrate it into an electronic health record. The U.S. government program of Meaningful Use is forcing the adoption electronic health record use in 3 stages by 2017. As always, encouragement is by reward initially, followed by penalty in the later stages.
Now as you sit in a doctor’s office, you are likely yourself talking to yourself rather to your doctor who’s not spending any face-to-face time with you. He or she is likely staring at a computer screen and typing notes as you speak. Because of physician shortages or need to meet RVU targets (unit measure of patient care), your doctor has 10 to 15 minutes to spend with you. During that time your doctor has to document all key elements of the visit and check off various measures Meaningful Use but if you are lucky, a minute will actually be spent on a limited physical exam.
Compare that with the experience you had when you were younger. Decades ago my old family doctor sat in front of me, talked to me and talked with me. He would jot a few notes on paper. I got an examination and a treatment plan. He made me feel as if I had spent a long time with him. I would call that “meaningful.”
As the government, health insurers and hospitals demand greater efficiency, more documentation and of course, error free care, it is in their best interest to replace us with machines. There will no longer be any medical errors, malpractice will become history, and your doctor won’t be exhausted or troubled with anything so trivial as feelings. Who needs that sort of interaction because you are only here for a service. In the near future, we will be talking to a computer with voice recognition. We won’t miss the warmth of a patient-physician relationship since that will have been bled from our experience and our memory. It would be like the depiction in the movie, Elysium, when Matt Damon talks to a computer rather than a human parole officer with hilarious results.
The human physician will become history. Laying of the hands will be replaced by computerized probing and touch sensitive feelers, not by doctors, but by providers.

I can hardly wait.
How Your Hospital Can Avoid A Nomination as a Great Place to Work
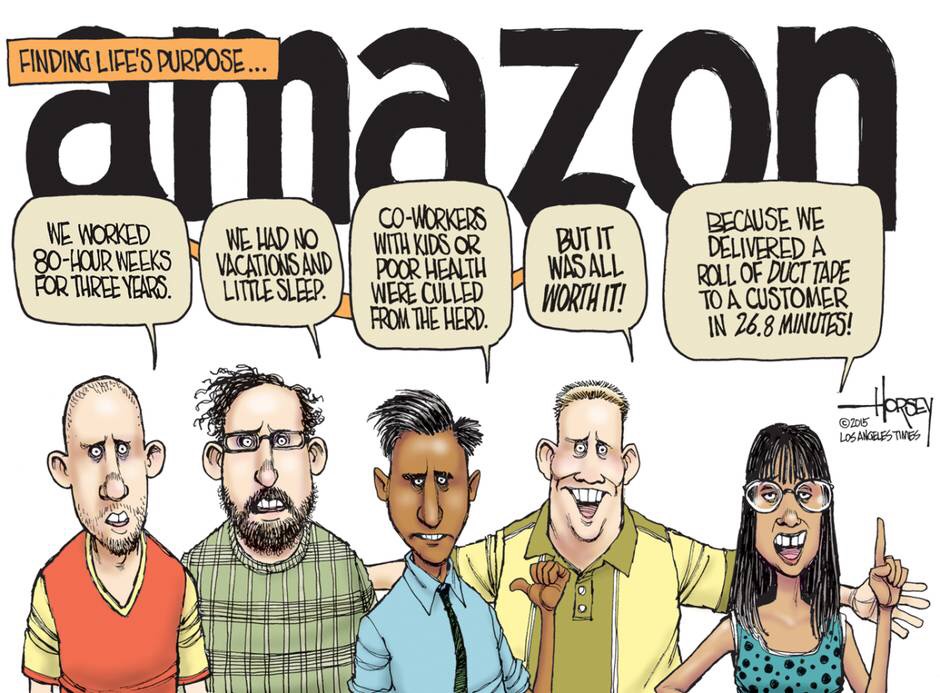 Image from Los Angeles Times
Image from Los Angeles Times
Earlier this month I read a Wall Street Journal article about Zeynep Ton's Good Jobs Index. Who is Zeynep Ton? She is a professor at the Massachusetts Institute of Technology’s Sloan School of Management who has ranked retailers on employee happiness. This was so positive. It was good to hear about businesses concerned about employee happiness and not just about profits and shareholders.
Two weeks later I was dismayed to read about the bruising work environment at Amazon in the New York Times. The article described a work environment toxic to workers overseen by a CEO who is blind to this view.
I was curious. I work in a hospital. Are hospitals ranked according to employee happiness? My health system is recognized as a Great Place to Work and the Fortune 100 Best Companies to Work For.
Last year I left a hospital that was an ideal model of health care in the President's eyes. Time Magazine had published two articles about that hospital. Yet my experience there as an employee was closer to the abusive atmosphere the New York Times detailed about Amazon.
I imagine that my old workplace could continue avoiding accolades from its employees by following these 14 steps:
1. Ensure there is a top-down management style. You cannot have middle managers like Department Chairs speaking on behalf of doctor employees. Instead just have the Department Chair spread edicts from higher up down to the masses. Upper management should remain uninterested in employee concerns.
2. Make sure there is no Doctors Lounge. That would only encourage restless employees to congregate and complain about management and the system.
3. Quarterly staff meetings should only be about the CEO and upper management decisions that have already been made for the employee physicians. Pretend to listen to employee concerns but remember, the meeting is really not about them but about upper management.
4. If any employee physician complains of burnout let them know they are welcome to leave and that they are replaceable.
5. Make sure that performance measures are impossible to reach and tie reimbursement and bonuses to these measures. By withholding monetary bonuses from doctors, think of the savings the system will accrue.
6. Since you really cannot measure or quantify caring, you should instead focus on irrelevant metrics that will frustrate your employees.
7. If your doctors stand up to patients by refusing to overprescribe narcotics or use antibiotics for viral illness, then when those doctors get poor patient reviews, make sure they are singled out to demean them and make them feel worthless. After all, great patient reviews are more important than providing great medical care.
8. Each year while the hospital cuts expenses, it should demand greater productivity from physician employees. When the doctors ask for more resources, more support staff or extra clinic time, tell them this is impossible because of expenditure cuts.
9. Take away coffee in the Operating Room nurses lounge because this will save the hospital money. That will have little effect on staff morale.
10. Brag that your CEO is a physician like many of his thousands of employees but make sure the employees know their place in the system by paying the CEO 40 times their average salary.
11. Remind your doctors it's more about numbers and quotas than patient care. If they do not meet RVU production targets their job is at risk.
12. When your doctors reach their 60s, don't treasure them. Instead find a graceless way to get rid of them. Younger docs are cheaper to hire. Remember that experience and wisdom are overrated.
13. Managers should set the standard for "work-life" balance by showing it is OK to ignore your spouse and children and OK to spend as much time as possible at work. The proper balance should tilt toward more work than life. Remind your workers the system is more important than family. The hospital is your family, 12+ hours a day. When you retire, you may find you have no family to go home to.
14. When doctors quit, don't perform exit interviews because you really don't care to know why they're leaving. You're just happy to get rid of them, so just show them the boot on the way out.
The lesson I learned was that I have to work in a Great Place, one that cares about its employees. If you are not in that great place, then leave.
Organizations should avoid pushing employees to do more and more in a thankless environment. A hospital should focus more on caring for patients and their staff and less about meeting quotas and upper management happiness.
My Venture Back to Microsoft – a Review of Windows 10
With the release of Windows 10 in late July this year I decided to wade back into the Microsoft waters. It had been six years since I last bought a Windows computer. I had grown to love the Mac OS and it’s simple beauty. I have lived with iMacs, MacBooks and iPads all these past years, but with the new Windows 10 release, I was intrigued.
But I was wary about taking the plunge. Two years ago I was forced to use a Windows desktop at a Sheraton while on vacation. I had to print boarding passes but I sat paralyzed in front of a bewildering Windows 8 screen. Where was the Start button? After clicking around For 1/2 hr, I managed to print the boarding pass.
The problem is that I work in a Windows environment. The electronic medical record I use is Windows based. Though I can connect to this Windows system through my MacBook Air laptop, the experience is clunky as it employs software called a Windows emulator.
So I began my research of Windows computers. I wanted portability so I decide to get a laptop. I liked the “2 in 1” machine which would allow me to use it either as a laptop or a tablet. I bought a Dell Inspiron 13 7000 with a 13.3 inch 1920 x 1080 touch screen, Intel i5 processor, 8 GB RAM, 500 GB hard drive for $649 at Best Buy. Despite the large screen, it weighed 3.6 lbs. Today Joanna Stern at the Wall Street Journal gave this laptop a thumbs up http://www.wsj.com/articles/windows-10-laptops-in-search-of-great-hardware-to-match-great-software-1439316432?mod=djemonwine_t
As expected I was able to connect to my Windows work environment without a hitch.
I began to play around with the Windows 10 operating system. The first thing I noticed was the annoying several second delay when waking the laptop from sleep. I would enter the numeric password, then have to wait and re-enter it, something I never saw with my Mac laptop.
Often programs such as Outlook 2013 would lock and display the “Not Responding” message, forcing me to close the program and start it up again. Again, this was unheard of on my Macs.
I played with the Siri-like assistant called Cortana and was at first frustrated – I recorded my encounter. Often Cortana would complain “the Internet and I are not talking right now” which hardly is a help.
After a few tries I got it to respond to the vocal command “Hey Cortana” but unfortunately she sent me to the Windows default search engine Bing. You see I had already made my preference browser Google Chrome instead of the new Microsoft Edge and I made the default search engine, Google within Chrome but nonetheless, Cortana would shoot my verbal inquiries into Bing. Cortana still has a long way to go before it can match Siri on my iPad and iPhone.
I bought the Microsoft Office 365 Family product ($80) at Best Buy a discount to the regular price only because I had bought my laptop there. Setting up my email with Outlook was tedious and certainly not as easily as I could do with my Apple products where I effortless can see my Hotmail, GMail, Yahoo and Exchange accounts. So far I have half those accounts working on the Windows laptop with Outlook. Whereas Apple allows for seamless integration across my machines, I can’t say I can do the same within Windows.
Flipping the screen around coverts the laptop into a tablet with a huge screen. The display is sharp and crisp. The touch screen is responsive but I found some of the regular Windows programs like Outlook were difficult to maneuver with my finger compared with a mouse or touchpad. I tried Flipboard but compared to the same app on my iPad, I found the Dell experience a little slow. I tried to play an embedded video in Flipboard on the Dell but the cursor just kept spinning. I opened the same article on Flipboard on my iPad and the video loaded immediately.
Is Living in Canada Better than Living in the US?
I was in Canada visiting my parents. I took a vacation from my job on the US East Coast. I often hear my US colleagues say how nice it would be to live in Canada, how the country cares for it’s people, provides lots of social services, just what a nice country should be. I grew up in Vancouver and after med school and working a while in Calgary, I moved to the US in 1992.
Here are some of my thoughts about the differences between the two countries. A lot of the hardship that seems more apparent in the US results from the fact it is a country of formidable size, so crime and poverty splash all over the news. Here’s some bad news: since I left Vancouver there seems to be as much crime as in the US – my mother lives in an upscale neighborhood and she has had several break-ins, as have all her friends. Despite the ‘free’ healthcare, downtown Vancouver is crowded with street folk who look as ill and unkempt as any you would find in Philadelphia or New York City.
As for the widely touted government funded social support in Canada, some say the social security there is more a trampoline than a safety net – rather than encouraging people back to work, many are content to collect unemployment benefits forever.
This government social network is tax funded which accounts for significantly higher costs of everything in Canada. I went to the grocer, Safeways, last night. A 3/4 pound bag of Starbucks which is $7-8 in the US costs $12 Canadian. A carton of Breyers ice cream is $4-5 in the US but sells for $11. The tax on beer is about 50% so a case of 24 varies from $26 to $38. Wine is very expensive. As for cigarettes, the price is enough to make one to quit for good. Gas is taxed to the lofty height of $6/gallon.
The only good news is that my family pays nothing for healthcare, not even a co-pay. Waiting is expected so when Mum had renal failure, she had to wait a few months to see the kidney specialist, but the consult and treatment was free, supported by the high taxes and high cost of everything.
Why the Healthcare.gov Site Failed
In the Time Magazine March 10 2014 edition there is an article on how the Affordable Health Care Act’s Healthcare.gov site was fixed.
When the healthcare.gov site was launched in October 2013, a mere hundred or so users caused the site to crash.
Typical of government led initiatives, the different sections responsible did not work in unison and there was no clearly identifiable person in charge of the site. Different parts did not know what was going on, so each assumed all was well and progressing forward. The Centers for Medicare and Medicaid (CMS) spent over $300 million on building a website that did not work. Their tech people forgot simple things like creating a cache, where most frequently accessed information is stored in a layer above the database. In that way queries could proceed quickly and not tie up the entire site – this is done in commercial sites.
The White House was forced to hire properly skilled tech folks from companies like Google to revamp the health care website. The newly hired consultants found that the original government designed site “hadn’t been designed to work right…that any single thing that slowed down would slow everything down.” Many of these troubleshooters fixed the site at a fraction of their usual pay. The lesson is that rich government contracts are awarded to incompetent cronies or to the lowest bidder. Since this is not a meritocracy, it’s unlikely that contracts would go to the most qualified at the onset. The good news for the government is that others can be hired later to do repairs.
Since originally there was no leader of healthcare.gov, we will never find out who was responsible for this mess and why so much money was wasted in the first place.
ProvenCare Rectal Cancer – the process begins
My hospital asked me to lead a quality initiative for rectal cancer using the ProvenCare model. ProvenCare uses evidence-based best practices to reliably give the best care to every patient. The goal is to reduce unnecessary variation in care, ensure all patients receive essential components of care and optimize patient outcome.
In 2003 Elizabeth McGlynn of the RAND Corporation published a study in the New England Journal of Medicine on the quality of care delivered in the US. Despite readily accessible standards of care in the literature, 45% of patients do not receive recommended care. This deficit in care is a threat to the health of Americans. It also represents unwarranted variation and inconsistency in care delivery, increases costs and affects clinical outcomes. Wouldn’t it be better if every doctor gave every patient the proper care at the right time, all the time?
My hospital rose to the challenge. With the help of a its electronic health record, it re-engineered the complex processes of care, reduced unwarranted variation and reliably delivered evidence-based care for specific diseases.
The ProvenCare model was first developed for elective coronary artery bypass grafting and hit the airwaves with revelation of a sort of money back guarantee. It has been used for bariatric surgery, hip replacement, cataract surgery, coronary stenting, lung cancer, with many other projects underway. Notably the lung cancer model was adopted by the American College of Surgeons’ Commission on Cancer and is being studied in 12 centers. The model came up with 38 elements of care based on evidence-based guidelines. Initial results show the initial six participating hospitals followed 90% of the 38 elements of care.
While some argue, mere compliance with process measures does not translate into better outcome, for many of the above diseases, Provencare has resulted in:
- Increased adherence to evidence-based guidelines
- Improved clinical outcomes
- Increased patient engagement
Rectal cancer represents a unique challenge. About 40,000 new rectal cancers are diagnosed yearly in the US and half will die from this cancer. While some may think most of these patients are treated at major cancer centers by colorectal specialists, only a small percentage receive such care. Most rectal cancer patients are treated by non-specialists in low-volume hospitals. As a result, there is a great variation in how the care is delivered and a great variation in the outcome. The literature shows that local recurrence can be as low as 0% and as high as 37%. Surgical mortality varies between 1.4% to 7% at the high end. The colostomy rate also varies throughout the country. Rectal cancer surgery is difficult as the cancer can be low, confined by a narrow bony pelvis. This can result in incomplete removal leading to local recurrence and death or hinder making an anastomosis (putting the rectum back together).
In addition to the surgical problems, patients should have high quality imaging of the tumor with either endorectal ultrasound or pelvic MRI but many hospitals do not have these tools. Some patients may need radiation and chemotherapy before or after surgery and may never receive it. Some could benefit from a multidisciplinary approach where each patient’s case is reviewed by a team of surgeons, medical and radiation oncologists and other providers. If that patient’s hospital does not have such a team, that team approach is not offered. After surgery accurate assessment of the tumor stage and the margin (how deeply the cancer invades the rectum) affects prognosis and treatment planning. Ideally this is best done by specially trained pathologists which can ensure the quality of the surgery.
So with a team of ProvenCare specialists, the rectal cancer project is underway. This plan will take about 40-50 weeks, with a meeting every week. The project is in 7 stages and presently we are reviewing the literature to identify the ‘best practices’ of rectal cancer care.
As each stage unfolds, I will continue to write about the process.
More Stupid Hospital Documentation Rules
Today I was notified by Medical Records at my hospital that one of my OR/surgery reports was incomplete. I had done hemorrhoid surgery on a patient 6 weeks ago. Someone in the medical records department flagged a deficiency in my OR note. I had left out the “drain” section – whether a drain was used or not. For my lay readers, you need to know that while drains can be used in abdominal surgery, I have never used one for hemorrhoid surgery in 27 years. In fact I can’t think of any colorectal surgeon ever using a drain for hemorrhoidectomy. In any case I was in violation as the hospital Medical Record Procedure Committee stated that Drain recording is a requirement and has to be addressed in the Operative report. I was directed to Rules and Regulations page 14. Was the documentation of drains a ‘requirement’ of the committee because of government regulatory agency rules or did the committee feel that drains should be used in hemorrhoidectomy? I doubt anyone sitting on this committee knows anything about anal surgery, so it’s likely a misinterpretation or misapplication of a badly written regulation. If this documentation of drains is required, then this should be mentioned in all surgery despite clinical relevance or common sense. Taking this to a ridiculous end in my hospital, drain use should be documented for anal fissure surgery, removal of rectal foreign body and colonoscopy performed in the OR in spite of logic that drains are never used in these procedures. It is thoughtless mindless enforcement of such ‘rules’ and regulations which lead to more and more doctors leaving medicine in frustration.
Patient Safety vs Just Culture
In a survey by the Agency for Healthcare Research and Quality’s (AHRQ) survey of hospital culture, some revelations came to light. It was disturbing that 26% of health care workers say whenever pressure builds up, managers want them to work faster, even if it means taking shortcuts. Fifty percent said they work in a “crisis mode”, trying to do too much too quickly and disturbingly, 36% report that safety is sacrificed to get more work done. Safety does not seem to be the priority when managers/administrators exhort workers to do more and overlook repetitive safety problems.
This is probably the tip of the iceberg. Each hospital is already under financial stress. They are placing higher unattainable financial targets in order to clear their overhead expense and try to break even what with the government cutbacks, increasing expense of business, etc.
It is hoped that with evolution in healthcare funding, there will be less emphasis on volume and more on good outcomes and results from the care delivered.
Complications can occur when a patient receives care. In fact, some patients develop a complication such as a wound infection after surgery. When that happens I don’t feel it is due to a mistake or error but many hospitals approach this in a punitive way. An email/letter is sent to the doctor but to get the point across it is also sent to the Department Head, Chairman of Surgery, and various administrators, so the complication is for all to view. All this does is make doctors reluctant to report errors.
Dr. Lucien Leape from Harvard in testimony to congress said, “the single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes.”
Only by developing a “Just Culture” and transparency like the airline industry where errors are reported without punishment will lead to improvement in healthcare safety. Continuing to push providers and punish the bad outcomes will leave healthcare mired in the last century.
